

A client has a new tank farm, and six (6) storage tanks are in identical service, and three (3) other are in identical service. So the question I get often is… Since these tanks are identical in their design AND service, can we use inspection data from one (1) tank to assess the conditions of the other tanks of identical design and service? The short and easy answr is YES, and here’s why…...
Read More
A summary of API’s 510 Inspection Frequencies:
(emphasis by me)
…
HomeRead More »
Read More
When classifying your piping circuits for MI/TML/CML inspections, DON’T share the inspection/NDE frequencies with the team!!! It is amazing to watch them “reconsider” their decisions after they learn the differences in inspection frequencies between Class 1 and Class 2. The exercise is to ENSURE the integrity of our PRIMARY CONTAINMENT (process safety); not to reduce costs!
Read More
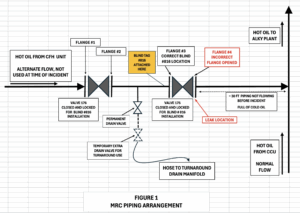
SAFTENG NOTE: The fatal H2S event in Deer Park last year that claimed two (2) contractor lives was the result of contractors opening the WRONG flange! Now we have a similar event that led to a fire that burned for three (3) days. A report regarding a 2025 Refinery Fire in CA found that two (2) contractors “mistakenly loosened the bolts on a flange full of hot hydrocarbons during a routine but...
Read More
Are you shocked this led to a fire? Welding on the wall of a boxcar that is full of paper goods. This is the exact set up OSHA warns us of… 1910.252(a)(2)(x) Noncombustible walls. If welding is to be done on a metal wall, partition, ceiling, or roof, precautions shall be taken to prevent ignition of combustibles on the other side, due to conduction or radiation, preferably by relocating combustibles....
Read More
The Compressed Gas Association (CGA) has published P-95, Guideline for the Safe Installation and Use of Cryogenic Food Freezing and Chilling Equipment. This publication covers the installation and operation of food freezing and chilling equipment and associated supply systems, and the use of that equipment with refrigerated liquefied gases (nitrogen and carbon dioxide). Topics covered in this publication...
Read More
At 4:30 p.m. on October 25, 2024, an employee, 53, was working on a crew with four (4) other employees fueling a boat when an explosion occurred. The employee died from 3rd degree burns to his body and blunt force trauma to his head. Four (4) other employees were hospitalized to treat multiple burns.
…
HomeRead More »
Read More
At 12:19 p.m. on September 18, 2024, Employee #1, 42, was cleaning the paper machine rollers with an air hose. While performing the task, the employee was caught between the top roller and the mat. The employee was crushed by the rollers, resulting in fatal injuries.
…
HomeRead More »
Read More
It’s hard to believe that 2025 is already at its halfway mark. Temperatures are rising and humidity is creeping in for many workplaces, so it’s time to start measuring, monitoring, and responding to high-heat working conditions. Don’t ignore this hazard simply because OSHA has not yet promulgated a standard. Do it for your PEOPLE, not for OSHA.
Read More
Fill out this form to ask a workplace safety and health or retaliation question or to request a letter of interpretation. Responses to questions will be sent within ten business days, but interpretation requests take longer. All responses are for informational purposes only, and do not constitute an official communication of the U.S. Department of Labor or OSHA. For an official response,...
Read More
If you don’t know me and are confused as to what makes me tick as a safety pro… it’s data! And not just any data – VERFIED AND VALIDATED DATA! And this leads me to “on-line reviews”. I hear a lot of people refer to these on-line reviews about vacation rentals, restaurants, and products. They are serious about convincing themselves “it must be ok, just look at all these 5 star reviews”. I’m sorry,...
Read More
This paper concerns refrigerant gases classified as Division 2.1 flammable gases under the Australian Dangerous Goods Code (ADG Code) or classified as Flammable Gas Category 1 using the Globally Harmonized System (GHS). It covers general work health and safety/occupational health and safety (WHS/OHS) duties, however, readers should check their legislative responsibilities at the state/territory and...
Read More